
Angelman Syndrome (AS) is a neuro-genetic disease characterized by microdeletion of the maternal inherited 15q11-13 region. For the first time in 1965, the British pediatrician Dr. The syndrome described by Harry Angelman is seen at a frequency of 1/15,000 – 1/20,000.
The leading findings of the disease are mental and developmental retardation, prominent speech disorder, epileptic seizures, and a constantly smiling face. Due to this typical facial appearance, it is also called “Happy Puppet Syndrome”. 80% of the patients have epileptic seizures, microcephaly and scoliosis.
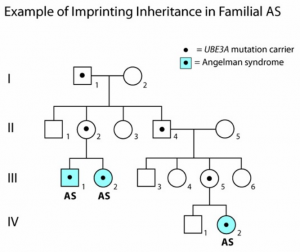
Another important cause of AS is the UBE3A (ubiquitin protein ligase E3A) gene mutation located at the microdeletion site and is responsible for approximately 5-10% of the syndrome. Other causes are 3-5% imprinting defect and 2-3% paternal uniparental dysomia.

HOW IS AS DIAGNOSED ?
The diagnosis of microdeletion, which is the most common cause of the disease, is made by the flourescence in-situ hybridization (fish) technique, which is a molecular cytogenetic method. There is no objective-objective method used for the diagnosis ofAS. The diagnosis of AS is generally evaluated by the pediatrician and geneticists between the ages of 3-7, where characteristic behaviors and characteristics become evident, as well as observation, developmental history and laboratory findings (genetic test results).
Timely diagnosis of AS poses a challenge for the clinician because there may not be significant dysmorphic features or specific clinical stimuli that easily indicate diagnosis during infancy. The behavioral phenotype is a crucial element in suspecting diagnosis, but this may not occur in a particular clinical encounter. Another challenge for the clinician is the multiple genetic mechanisms that cause AS, each disrupting UBE3A. Accordingly, several diagnostic genetic tests may be required to confirm the diagnosis.
Developmental delays are first noticed at 6 months of age; however, the peculiar clinical features of AS do not appear until after 1 year of age and it may take several years for the correct clinical diagnosis to be made. Diagnosis is often initially suspected on the basis of the behavioral phenotype, especially on the basis of combinations of movement disorder, absence of speech, and happy attitude. Although there may be marked mild craniofacial dysmorphism in some individuals with AS, diagnosis is rarely suspected based on these findings.
EARLY DIAGNOSIS IS IMPORTANT!
Early diagnosis is important for the start of special education, active and personalized physiotherapy and rehabilitation program as soon as possible. Early intervention positively affects language and social behaviors and is very important in solving the problems in motor development.
Clinical Symptoms in Angelman Syndrome
- Developmental delay (6-12 months)
- Speech disorder with little or no use of words; nonverbal communication skills higher than receptive language skills and expressive language skills
- Movement and balance disorders (usually gait ataxia), feet standing apart, legs shaking, jerky body posture, uncoordinated movements
- Behavioral uniqueness, including any combination of frequent laughter / smiling; open happy attitude; excitement, usually by clapping of hands; hypermotoric behavior; short attention span.
- Delayed or disproportionately slow growth around the head usually results in absolute or relative microcephaly by the age of 2.
- Seizures that usually start to occur before the age of 3
- Abnormal electroencephalogram (EEG) with characteristic pattern of large amplitude slow pointed waves.
- Nutritional problems in infancy,
- Hypopigmental skin and eyes (60% of children have less pigment than normal in their skin, hair and eyes. Their skin is pale and easily damaged by sunlight. Lack of pigment in the eyes may cause problems such as eye shift and visual impairment.)
- Tongue, sucking and licking problems, tongue being larger than normal and outside, frequent drooling
- Excessive oral and chewing behavior
- Hyperactive lower extremity deep tendon reflexes.
- Particularly during the ambulatory lifted, bent arm position.
- Wide-bottomed gait with outgoing (i.e. pronated or valgus positioned) ankles.
- Increased sensitivity to heat.
- Abnormal sleep-wake cycles and reduced need for sleep.
- Water attraction / admiration; admiration for wrinkled items such as certain papers and plastics.

AS And Eating Problems
Hand sucking is commonin infancy, and as it grows older, it is replaced by a fondness for chewing and oral stimuli. The problem in the tongue and mouth structure can cause problems in skills such as chewing and sucking. Exercises to develop oral-motor skills help solve eating and salivation problems. Eating problems decrease with age.
AS and Hyperactivity
Hyperactivityis frequently seen in childrenwith AS.
Hyperactivity, which is seen especially in early ages due to short attention span, affects girls and boys at the same rate. It is seen that babies and children act carelessly, constantly put their hands and toys in their mouths, and they cannot take care of an object for a long time and pass from object to object. Biting, pulling and pinching behavior in older children is related to hypermotoric activity. A continuous and consistent behavior change program produces positive results in reducing or eliminating unwanted behavior. Research shows that hyperactivity decreases with age.
AS and Balance Problem
Theretardation ingross motor development is observed as a balance problem around 1 year of age.The child learns to sit without support around 13 months, to lift and push himself forward around 22 months, and can start walking between the ages of 2-7. A small proportion of children cannot walk without support. Muscle tension seen at an early age is another cause of balance problem. While mild cases may start to walk normally, in severe cases, walking like a robot or unable to walk at all due to stiffness in the muscles may occur.
AS and Communication
They are open to communication and close to people frominfancy. The short attention span negatively affects interaction and communication. All children with AS have speech problems. Oral-motor problems cause eating problems as well as affect speech. Some of them don’t talk at all or speak in a limited number of words. Receptive language (understanding what is communicated to them) is always better than expressive language (expressing their needs). Alternative communication approaches such as sign language and communication with pictures are frequently used in these children.

Treatment and Therapy Approaches
There is currently no definitive treatment forAngelman syndrome. Therefore, the treatment focuses on symptom management. Educational therapies are used to increaseadaptation and skills and to eliminate some symptoms. Many of these are behavioral therapies.
Educational approaches such as physiotherapy, work and occupational therapy ,speech therapy, hydrotherapy , musictherapy to improve motor , language and social skills support the development of the child.
Children with AS often need highly structured activities and routine creation because they are hyperactive and have concentration problems. In environments where there are too many warnings, they exhibit hyperactive behaviors. Mobility and stereotypical behaviors decrease in structured and controlled environments.Anxiety caused by inability to understand and express oneself may cause frustration. Determining the child’s communication skills and forms by a speech therapist is useful in teaching the child one of the most appropriate communication methods (sign language, communication with pictures and symbols… ) and thus reducing behavioral problems.

TEACCH (a visual, concrete communication method that facilitates interpersonal communication) is one of the methods used to gain daily life skills and self-care skills. TheTEACCH program aims to make the physical environment, daily programs, individual working systems understandable for individuals of all ages and levels of functionality by using visually structured teaching techniques. The main purpose is to improve the child’s communication and to ensure that he/she lives as independently as possible.
Structured programs remind the child who has difficulty in following the order of the work he/she will do, enable a child with insufficient receptive language to understand the verbal instructions, show the order of the works to be done to the child with a weak auditory memory, allow the child who is frequently distracted to look at and focus on his/her program, being in the program of the activities he/she loves increases the motivation for him/her to do what he/she needs to do as soon as possible, and reduce the anxiety created by the unknown because it eliminates the unknown.
Occupational therapy is necessary to stimulate fine motor and verbal-motor control skills.Speech therapy involving non-verbal communication methods, picture cards or communication boards should be initiated because active communication in this group of children is poorly developed. Since they are interested inpeople and their receptive language is developed, they can share responsibilities and establish friendships in daily life. Starting from the early years, structured game play should be supported and they should benefit from special education and inclusive education.
The healing effects of the game
- Self-Disclosure
- Revealing unconscious conflicts
- Learning and overcoming knowledge and skills deficiencies directly
- Being able to gain power and control in his/her life
- Anxiety that may arise in the face of stressful events can be reduced by acting out in advance.
- It allows repressed emotions to be expressed.
- Sense of empathy
- Being able to make his/her own decisions and discovering himself/herself
- Strengthening the emotional bond between parent and child
- Creative problem solving, making discoveries
The Importance Of Physiotherapy In AS
IN AS, Physiotherapy is required to solve problems related to joints, to support joint mobility, and to prevent contractures.Involuntary, irregular movements can prevent walking, feeding, and reaching for objects. The retardation in gross motor development is one of the reasons that delay walking. Hardness or tremor in the child’s legs may cause impaired gait. Physiotherapy is a supportive method in the treatment of all these problems.

Clinical Evaluation In AS
Coarse Motor Function Classification System (GMFCS)
The level of disability was determined using the coarse motor function classification system. Classifications range from I (independent mobility, but some minor speed, balance, or coordination difficulties) to V (no independent mobility, physical disruption restricts voluntary control of motion and postures against gravity). GMFCS is widely recognized and used as a way to categorize motor function in children with cerebral palsy (SP) and some other children with pediatric disabilities such as AS.
Level 1: Walks without restriction.
Level 2: Walks with restrictions.
Level 3: Walks using handheld mobility tools.
Level4: Self-movement is limited. It can use the motorized mobility vehicle.
Level 5: It is carried in a wheelchair that is pushed by hand.
Gross Motor Function Measurement (GMFM)
GMFM will be suitable for children whose motor skills are equal to or lower than that of a 5-year-old child without any motor disabilities. This test scores how individual motor movements and postures are compared with specific identifiers and records the change over time.
Gross Motor Performance Measurement (GMPM)
Gross motor performance was developed to assess the quality of movement and the change in time in children with DEC december age range from 5 months to 12 years.
MODIFIED ASHWORT SCALE
Spasticity is measured.
0 : No increase in muscle tone.
1 : At the end of the range of motion, there is a slight increase in muscle tone characterized by capture and relaxation or a minimal resistance.
1+ : There is a slight increase in muscle tone characterized by minimal resistance over less than half of the range of motion.
2 : Joints can move easily, but there is a greater increase in muscle tone throughout the entire range of motion.
3 : There is a significant increase in muscle tone that makes passive movement difficult.
4 : The affected joint is completely rigid in flexion or extension.
Berg Balance Scale
Balanceis the main component of ambulation. Berg Balance Scale (BBS) is an indicator of balance and motor skill in the average independent walking age. It consists of 14 items.
Physiotherapy and Rehabilitation Therapy in AS
Focuses on the patient’s goals and follows a problem-based approach to address symptoms and comorbidities.
Neurodevelopmental Treatment (Bobath Concept)
TheBobath approach is one of the closest and most effective treatment approaches to the child’s nature today in terms of correct holding techniques, positioning, encouragement of movement, importance given to the family and teamwork in treatment and, more importantly, putting the family exactly where it should be in treatment, taking into account the child’s current situation.He/she tries to examine the central nervous system by knowing the normal motor development steps very well. As a result, it reveals the finding caused by the problem in the central nervous system with comprehensive evaluations. Then, it determines the needs of the child and implements the requirements of the concept accordingly. While doing this, he approaches the child by seeing the whole picture. In other words, it approaches the situation
holistically. Within theconcept, it can be supported by methods such as equine therapy (Hippotherapy), pool therapy (Aquatherapy), sensory integration therapy, kinesiotaping and theratogs, while adhering to the main purpose of treatment within the needs of the child.
The use of orthosis and adaptive auxiliary devices is very important in the Bobath concept. Treatment should be supported by methods such as botox and serial plastering to help regulate the correctly selected orthosis and tone in line with the need. In this way, possible musculoskeletal problems will be reduced or eliminated. Exercises can be given to increase the mobility of patients to prevent contractures .These exercises can also increase gross motor skills. Jumping, running, cycling, throwing an object, catching, kicking a ball, etc.


Balance training: Studies suggest a protocol where the patient sits or stands on different supports and should use upper extremity functions. For example; while working on the balance board, the ball can be thrown into a basket opposite at the same time or the ball can be played with the physiotherapist. If the patient has difficulty in balancing, s/he can draw, paint, etc. activities by getting support from a table or bed. Standing on one leg and walking on the line can also be done.

Posture and scoliosis should be evaluated carefully Good management of posture from an early age can prevent or alleviate scoliosis. Physiotherapist and adult therapist may be consulted from time to time for advice on posture and sitting, including during adulthood.
Respiratory training: Cardiorespiratory training is required, especially in individuals with severe scoliosis. It may be preferred to make breathing exercises enjoyable with some toys and auxiliary equipment rather than working directly in children.


By giving exercises that increase fine motor skills, grip skills are increased and thus it can be facilitated to perform daily life activities. Stringing beads, using scissors, writing, buttoning buttons, stringing pasta on a straw or string, etc.


Studies to develop oral motor skills reduce the child’s language and eating problems. It is also necessary to solve problems such as swallowing and chewing problems, weakness in mouth awareness, speech problems and weakness in saliva control.
Alternative Therapies
Hippotherapy Therapy is facilitated by the horse using horse movements. Hypotherapy has been reported to improve speech and language skills as well as posture, muscle tone, coordination, balance, and sensory/motor development.
Hydrotherapy : Water-based treatments have been successfully used to manage symptoms in individuals with AS due to their love of water.
Cycling-static and trikes: A maintained exercise routine can be extremely beneficial, and many families of Angelman syndrome in particular have found that caregiver-controlled bicycles are invaluable.
Music therapy: Music therapy has been used to help people with learning disabilities express their thoughts and feelings and communicate meaningfully with others.
Body brushing has been used to amplify reflexes and stimulate nerve endings in people with learning disabilities.
Reflexology :Reflexology (massage or pressure on certain parts of the feet that are believed to correspond to other parts of the body) has been described as a useful, non-invasive approach to therapy for people with learning disabilities.
Aromatherapy
Many people with AS enjoy the sensory touch and olfactory experience, and this approach can help with relaxation, collaboration, and listening, among other benefits.
Cranial osteopathy
It is a technique in which the bones of the skull are manipulated. Scientific studies have not proven the usefulness of this technique in AS. Some parents have reported that it reduces hyperactivity and improves sleep.
Leave a Reply